At PCC, we are monitoring the impact of COVID-19 on our clients' practices every day, all day (hence this late blog tonight). With the help of Tim and Alex at PCC, we're gathering customer data daily and looking for patterns that might steer us away from the rocks or simply to smoother waters.
I've had a lot of questions about how COVID and, in particular, telemedicine, is affecting E&M distributions among pediatricians.
- How are visit patterns affecting the typical 99212-99215 work? Are patients coming in for more or less complex service?
- For video visits using 9921X codes, what are the typical patterns? Right now, the world has no idea, so this is the first look into actual telemedicine coding that I'm aware of.
- For phone visits (that's 99441-3 and 98966-8), what are the typical patterns? How is phone usage evolving? Don't you want to know if you are over- or under-doing it?
Let's look.
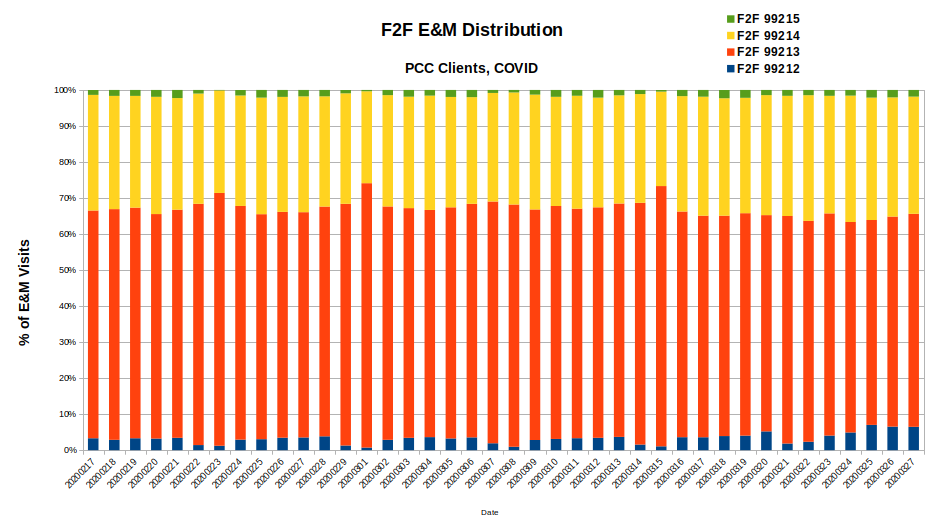
Here is the 99212-99215 distribution for practices dating back to mid-February. Squint a little if you need to...the red portion of is bar is the 99213, the small blue section at the bottom are the 99212s, the yellow is for 99214, and our often invisible friend, 99215, is at the top.
For the entire period, there is remarkably little movement. However, note that the last week or two has seen a small increase in 99212s, small increase in 99214s, and an almost immeasurable increase in 99215s. Nothing revolutionary, however.
Let's take a look at the video visits.
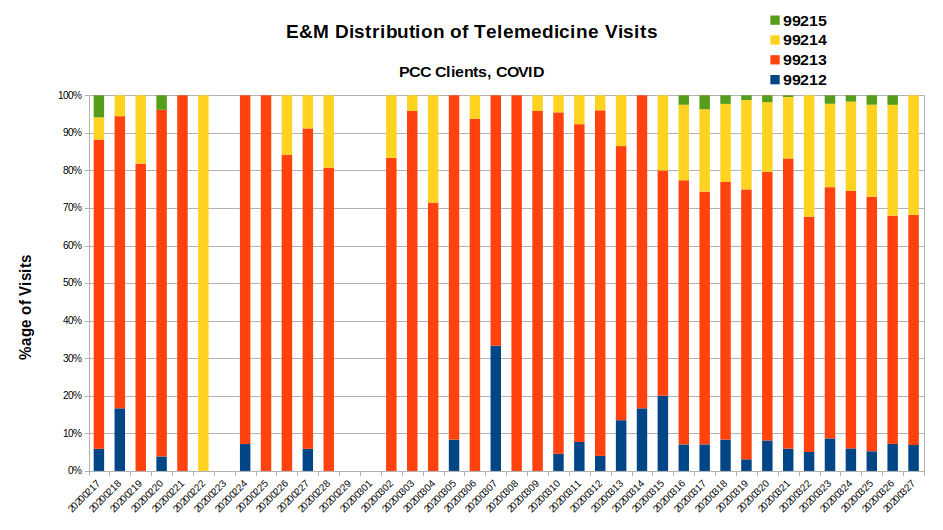
Ah ha, here we see some patterns. First, the 99213 is a LOT more prevalent, as is the 99212. The 99214 is somewhat squished but growing. Sample size is an issue, but it looks like there might be a slight boost in 99215s.
One issue to consider is that a number of payers are not recognizing 99214s or 99215s for video visits even though they are approved by Medicare. There's only one reason to have that limitation: greed. If you spend 45min on the phone counseling one of your patients on an important clinical matter, you may max at a 99213. Sigh.
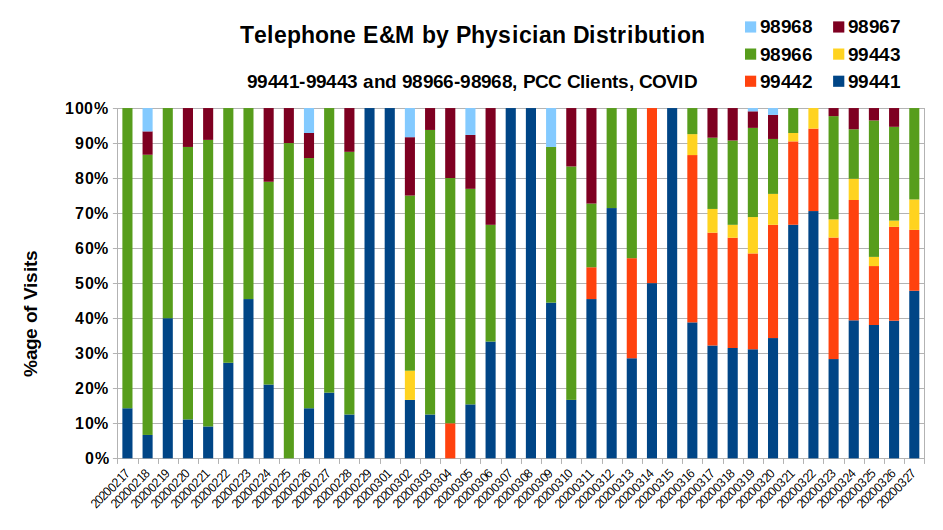
I also wanted to look at the distribution of both the phone and 'digital' (i.e., portal and email) codes. Turns out that the volume of digital codes being billed by PCC clients is so low that I don't trust it. We get just the phone codes as a result:
I'm mixing these together for now, I may split them up as they grow.
Remember, the 99441-99443 is for PHYSICIANs and the 98966-98968 is for "qualified nonphysician health care professionals." That latter item is defined differently from locale to local (i.e., does it include MAs, RNs?). Nonetheless, here's what you can learn from this chart:
- a couple weeks ago, the 98966 (let's name it a "nurse call") was the primary billed phone event for our clients - you can see it there in green. It doesn't mean there were a lot, just that it was the most common.
- when COVID really hit practices, you see an immediate spike in the 99442 (11-20 min on the phone with a doc).
- weekends have very different behavior, apparently many of the calls are easier (see the spikes in 99441 that appear like clockwork).
- I'm not surprised to see the 98968 disappear - that's the 21+m phone call with the non-docs. At this point, I think those calls are being handed to the physicians for a higher chance of being paid.
We have plenty more work to do and I'm aware of the limitations of this data, but PLEASE ask me questions and we'll do our best to answer.
In the meantime, if you want to be notified whenever I send out a post like this, subscribe in the box there in the upper right. Also, join the COVID-19 forum that Paulie and I are hosting. To date, it's the best, central source for COVID-19 information for independent pediatricians.
Comments
13 Comments