This blog is going to raise more questions than it answers, but one let's get one of the few clear answers we have out of the way: pediatricians do not appear to follow Bright Futures' periodicity schedule for developmental screening. I realize that may not shock many of you, but you might be shocked to see how far apart the standard of care and the recording of that care really are.
A little background: at PCC, we are working on expanding the clinical measure aspect of our dashboard and we got the "bright" idea to provide feedback relating to the BF periodicity schedule. Experience tells us that there is a wide range in the delivery of such simple and understood necessities as vision and hearing screening that we expected developmental screening to have similar challenges. In other words, where we expect to see a vision and hearing screen performed at, say, every 4y and 5y visit, we simply don't. And that, IMO, is crazy. At PCC we want to fix the issue of clinical inconsistency and missed opportunity - we want every child to get the entire suite of BF expected services. It's good medicine and it's good for the practice.
Developmental screening has three expected appearances in early childhood - at 9, 18, and 30 months. At each of these visits, we should see a 96110 CPT. What do we actually see?
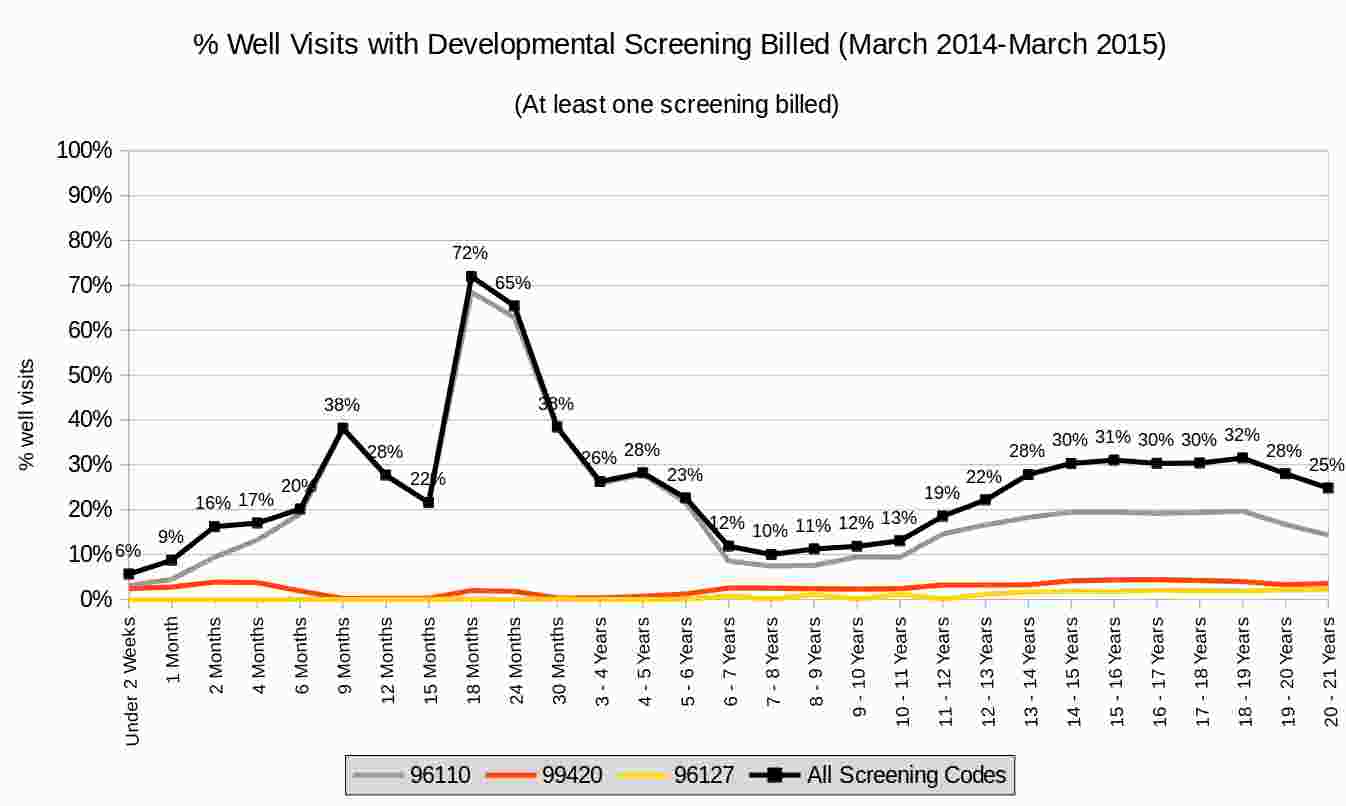
Click on the image if you want a closer look, but the story being told here is that pediatricians record a 96110 at only 38% of all 9m old visits, 72% of all 18m visits, and 38% of all 30m visits. What's going on here? As I said, this raises more questions and provides answers, but here are some details of the data for those who want to drill into it:
- Sample size? ~800,000 well visits over the last year, so that's not really an issue. And these are better-performing practices.
- We are aware that some practices are using a 99420 (either out of necessity or mistake), so we've included that code just to be safe. We also know that a minority of practices are already using the new 96127 code - and even though that's supposed to be for behaviorial screening specifically (i.e., your Vanderbilts), we threw that in too.
- We are only measuring how often the developmental screening codes are billed - we aren't measuring how often they are recorded in the EHR or performed and not recorded. This difference is subtle, but important. Ultimately, we are underestimating the real use of this service, but probably not enough to explain what's going on.
- What is going on? Clearly, pediatricians have some understanding about using developmental screening tools in the 18-24m time frame, but that's about it. Yes, there's a measurable jump at 9m, but those pediatricians are still in the minority. And we've heard from a number of our clients who explain that they don't do the 30m visit (for a variety of reasons, none of which I support), so they squeeze in another screening at 24m.
- I know a number of practices who don't like any of the billable tools, so they use a variety of their own screening methodologies. I understand why they do this, but I can't support the use of non-standardized tools. But don't take my word for it, listen to the pros.
I'd like to hear from anyone who can shed some light on what we see here.
Comments
18 Comments