Need proof that this is the best pediatric practice management resource on the planet? Check it out.
Oh, first: major drama at PCC's office last night. Let's hope this post is the closest I come to being a war correspondent. I don't like the proximity of the event to yesterday's message about flooding.
Meanwhile...Igor and I were doing some work on our [secret project, still] and were looking at E&M distribution among pediatricians. Here's a trick question - should 9921X codes that result from an initial well visit be counted as part of your distribution? Most people say yes - but I'm not convinced. Sick codes discovered during well visits should, by their nature, have a different distribution. It's not as if, for example, Mom waits until next week for her scheduled physical to talk about that seizure or red, sore throat (ok, some wacky ones do, but you get the point). 99214s and 99215s come to the office as a rule. I believe that -25 modified codes will have a different distribution. I'll post the results later.
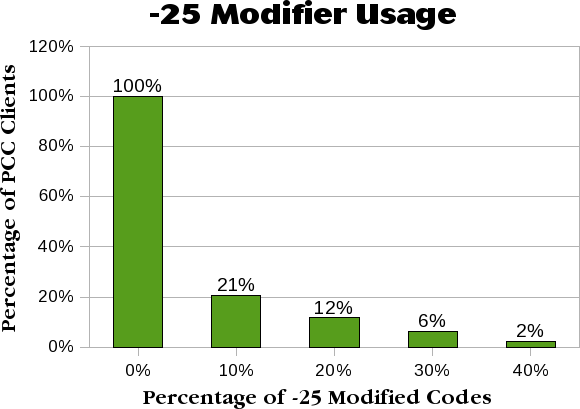
What we did look at, though, is how many pediatricians actually use the -25 modifiers in the first place and how often they do. Here it is, data you can't get anywhere else:
What this shows is that 2% of our clients put -25 modifiers on 40% (or more) of their E&M codes. 12% put it on 20% or more. Get it?
What the chart doesn't show is that 22% of PCC's clients never use a -25 modifier.
That's crazy. Especially when you consider the fact that we have good customers. So, how about you? How many of your E&Ms have -25 modifiers?
{kind=link}